
ALLOPREGNANOLONE ………………………………………….float high above your clouds
Allopregnanolone is a hormone made from progesterone in the brain: thus it is a “neurosteroid” hormone.
It works with progesterone, melatonin, vitD and T3 to perform cleanup, maintenance and repair, for the brain.
I refer to it as the brain’s “housekeeper” (see the page on Alzheimer’s disease).
- It facilitates removal of metabolic waste from the brain, during sleep.
- It is active in brain maintenance and repair: it stimulates production of “BDNF” (brain–derived neurotrophic factor), which encourages production of new brain cells and interconnections (“synapses”) between new cells and old ones.
- It works with progesterone, melatonin and thyroid hormone (“T3”) to wrap the nerve fibres with myelin, which insulates them and thereby permits passage of electrical signals.
- It is antidepressant: it is the reason that “SSRI”antidepressants work – SSRIs increase production of Allopregnanolone and it is the Allopregnanolone which relieves depression. (6)
- It reduces anxiety and in so doing, relieves “perceived stress”,* thereby improving Thyroid hormone function.
- It reduces our tendency to aggression and encourages production of oxytocin, the hormone which increases our “friendliness” and the “warm and fuzzy” attitude we need for social and sexual interaction.
- Allopregnanolone puts us to sleep (for sleep, it is more important than melatonin).
- It enhances our thinking ability and facilitates formation of memories.
- It reduces perception of pain by generation of “endorphins”, our internal painkiller.
- In conditions in which myelin has been lost from the nerve fibres, allopregnanolone, progesterone, DHEA and T3 can work together to re-myelinate the nerve fibres.
Wikipedia refers to Allopregnanolone as “stress reducing, rewarding, prosocial, anti-aggressive, pro-sexual, sedative, sleep facilitating, pro cognitive, memory enhancing, analgesic, anticonvulsant, neuroprotective and neurogenic”. (4)
During pregnancy, Allopregnanolone acts along with Progesterone, DHEA, Testosterone and Triiodothyronine (Thyroid 3), to reduce the mother’s perceived stres and to relax and calm the baby; but more importantly, it is active in the normal development of the baby’s brain and nerves. (4)
Deficiency of Allopregnanolone, DHEA, Testosterone and Triiodothyronine (T3) leads to mood swings and anxiety: Allopregnanolone deficiency by itself can cause premenstrual dysphoric disorder (PMDD, PMS), postpartum depression, major depression, anxiety disorders, catamenial epilepsy and other neuropsychiatric conditions.
However all of these distressing conditions are worse when DHEA, Testosterone and T3 are also low.
Progesterone is converted to Allopregnanolone, which works with DHEA and T3 promote neurogenesis, neuronal survival, myelination, increased memory, and reduced neurotoxicity (2). Therefore treatment with intravenous Allopregnanolone
(or Progesterone, given transdermally, vaginally or orally) has been used to relieve postpartum depression, major depression, TBI (traumatic brain injury) and stroke (CVA).
Potentially, Allopregnanolone should be helpful in stabilising neurological diseases, including MS, Parkinson’s and Alzheimer’s disease, but that has not been proven.
NORMAL CIRCULATING LEVELS OF ALLOPREGNANOLONE
As noted by Genazzani et al. in 1998 (1) (see Fig.1), Allopregnanolone levels vary with age and gender.
During the menstrual cycle the Allopregnanone level follows that of Progesterone and in pregnancy, Allopregnanolone levels increase along with progesterone and DHEA (1).
In young males, the level is the same as in females during the first two weeks of the menstrual cycle, but it falls gradually from age 26 and can approach zero, in old age.
In postmenopausal females, Allopregnanolone is at young-male levels, but further age-related reduction is very slow.
Production of Allopregnanolone is increased by stress relief: fun, laughter, rest, sleep, alcohol, tranquilizers, antidepressants, meditaton.
See figure 1, for gender and age comparison and figure 2, for Allopregnanolone levels in the menstrual cycle (1). In each age group, black shows the men’s values and white, the women’s (fertile women in the follicular phase, before the ovary releases an egg) ***.
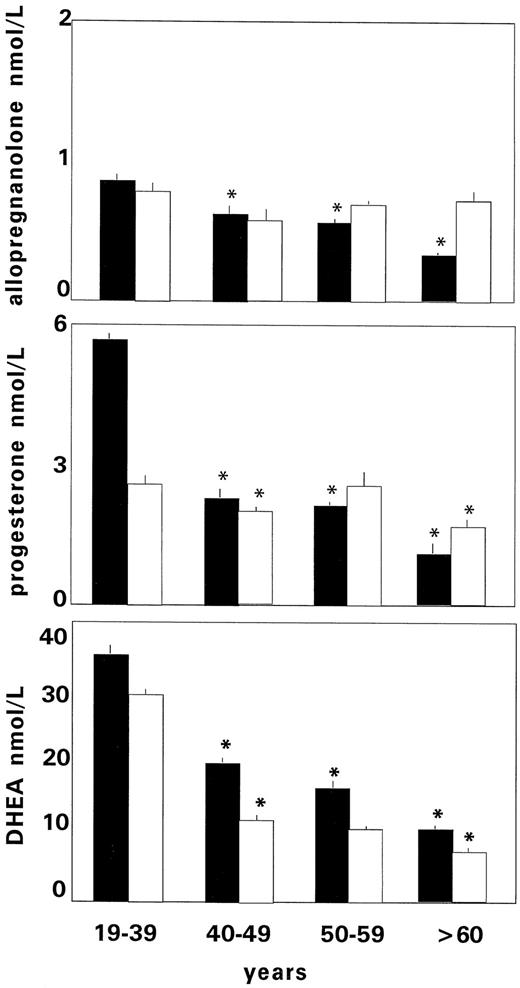
Figure 1, from Genazzani AR, et al. The Journal of Clinical Endocrinology & Metabolism, Vol 83, # 6, 1 June 1998: https://academic.oup.com/jcem/article/83/6/2099/2865559
In females the level of Allopregnanolone parallels that of progesterone (Fig.2, from Genazzani et al), being lowest (approximating adult male levels) during the menstrual “period”, remaining low in the follicular phase (2nd week) of the cycle and increasing to a maximum in the luteal phase (15th – 24th day).
Figure 2. Allopregnanolone (•), P (▪), and DHEA (▴) levels during the menstrual cycle, providing that Progesterone is normal).
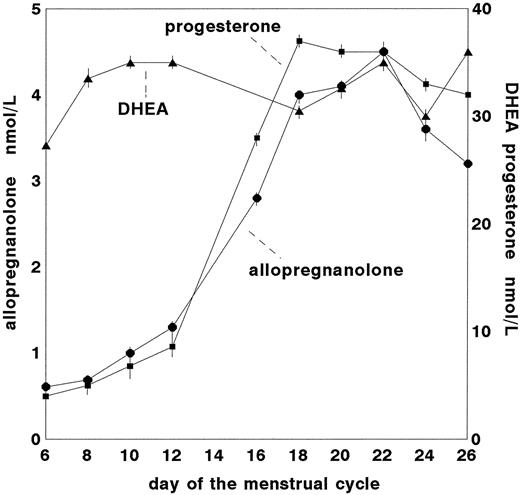
Figure 2, from Genazzani AR, et al. The Journal of Clinical Endocrinology & Metabolism, Vol 83, # 6, 1 June 1998: https://academic.oup.com/jcem/article/83/6/2099/2865559
DEFICIENCY of ALLOPREGNANOLONE:
Since Allopregnanolone is made from progesterone, a deficiency of Allopregnanolone will exist whenever progesterone levels are subnormal.
Many young women are progesterone under-producers, so deficiency can begin at any age, but there are two groups: Those deficient ab initio and those in whom progesterone underproduction results from steroidopenia **.
There is a tendency to suppression of Allopregnanolone production by stress, leading to depression and reduced neurogenesis, which may result in failure to achieve optimal brain development in situations of chronic stress. (5) This hypothesis, as yet unproven, would explain the reduction in cognitive ability among the socially disadvantaged.
Reduced progesterone and Allopregnanolone production is seen in postpartum depression, major depression, anxiety disorders, premenstrual dysphoric disorder, impulsive aggression, schizophrenia and autism.
In the PMS group, progesterone is lower and DHEA higher in both follicular and luteal phases of the menstrual cycle and free testosterone is higher in the luteal phase. (Since DHEA and free testosterone fall rapidly beginning at age 26, this statement is valid only for females in the 2nd and 3rd decades).
In PMS sufferers, Allopregnanolone & progesterone are low and DHEA & testosterone are high, in the luteal phase.
This explains the anxiety, aggression and irritability reported by young PMS patients.
In the autism spectrum, reduced Allopregnanolone production parallels the severity of the condition.
SUPPRESSION OF ALLOPREGNANOLONE:
An enzyme called 5-alpha reductase performs the process of changing progesterone into Allopregnanolone, so any drug which blocks 5-alpha reductase suppresses Allopregnanolone production. One drug which does this is FINASTERIDE, used to shrink enlarged prostates and to treat hair loss in men.
Unsurprisingly, the major side effect of finasteride is anxiety, depression and suicidal attempts.
ENHANCEMENT of ALLOPREGNANOLONE:
Any relaxant or antidepressant drug or activity will raise Allopregnanolone levels, including tranquilizers, antidepressants, music, yoga, meditation, alcohol and laughter.
This may be the reason (mechanism) for “miracle cures”, “healing by prayer and belief”, as well as the improvement in chronic disease sometimes credited to the “snake oil salesman”.
HORMONE RESTORATION THERAPY
Currently, there is no easily available Allopregnanolone preparation. The proprietary product, “Zulressa” is bioidentical Allopregnanolone, but has only been prepared for intravenous administration and vaginal application (as a cream). Currently, it is used for postpartum depression. It seems reasonable to assume however that the vaginal cream would control or ameliorate conditions caused by Allopregnanolone deficiency, including depression
SUMMARY
Allopregnanolone, a neurosteroid derived from progesterone, performs brain and nerve maintenance and repair.
Its assistants are pregnenolone, progesterone, DHEA and triiodothyronine.
Adequate production of this hormone guarantees good “mood”, tranquillity and optimised cognition, but remember that Allopregnanolone production falls when DHEA, Testosterone, Progesterone or Thyroid-3 levels are too low.
Women produce much more Allopregnanolone than men do, in the 2nd fortnight of the menstrual cycle and during pregnancy and tend to anxiety/depression when their Allopregnanolone production falls.
The slowly progressive reduction of neurosteroid biosynthesis, including DHEA, progesterone and testosterone, which begins at age 26 in both men and women leads to a reduction of Allopregnanolone synthesis, which contributes to the development of “psycho-cognitive loss”: anxiety/depression, fuzzy thinking, memory loss and confusion (6).
This condition mimics early Alzheimer’s disease, but is easily reversed by hormone balancing: supplementation of DHEA (which reliably increases Testosterone), Progesterone (which is converted to Allopregnanolone), Thyroid 3 hormone (which increases the efficiency of all cells, including brain cells) and in the menopause, Estradiol.
Allopregnanolone levels are decreased in stress‐induced psychiatric disorders, including depression and post‐traumatic stress disorder (PTSD), cognitive decline, neurological diseases including Alzheimer’s and MS, traumatic brain injury, stroke and chronic diseases generally.
Elevating Allopregnanolone levels by prescribing progesterone and/or pregnenolone, with DHEA and T3 as necessary is a valid therapeutic approach to counteract behavioural/cognitive/psychological dysfunction in many cases.
Remember: most people suffering from Allopregnanolone deficiency are also deficient in many, or all, of the neurosteroid hormones, so the entire range of hormones should be assessed and restored to normal levels.
Progesterone, also by mouth, provides the raw material for making Allopregnanolone.DHEA produces effects similar to those of Allopregnanolone in two ways: via production of Testosterone and by acting as raw material for micro-hormone production throughout the body, including the brain.
Triiodothyronine (“T3”, the active form of thyroid hormone) is also essential to cognition, mood elevation and general well-being, because it optimises cell efficiency and without it, all functions slow down.
Melatonin and Vitamin D3 (actually a hormone, not a vitamin) assist Allopregnanolone in its work.
Music, meditation, alcohol and CBD aid Allopregnanolone production, which is why they improve mood.
* Some stress may not be recognised as such by the individual, but subconsciously registered and reacted to by the brain. “Perceived stress” is stress which is high enough for the subconscious brain to recognise it.
** “penia” means “shortage of”, so “STEROIDOPENIA” is “low neurosteroid level”.
*** see also the page entitled “PROGESTERONE”
TREATING ALLOPREGNANOLONE DEFICIENCY
Currently, a synthetically produced, but bioidentical Allopregnanolone called Brexanolone (trade name Zulresso) has been approved by the USDA, for treatment of postpartum depression.
BREXANOLONE, given intravenously because it is poorly absorbed via the oral route, can be expected to be effective for Allopregnanolone-deficiency depression.
However its effect will be short-lived unless the stress reduction it produces translates into relief of the functional hypothyroidism and resumption of Allopregnanolone production: this cannot be guaranteed.
ZURANOLONE, a synthetic, orally absorbed, non-bioidentical analogue of Allopregnanolone, is in the trial phase.
it is unlikely however, that Brexanolone or Zuranolone will produce a permanent “cure” of depression (and particularly, PFS) by themselves, because the reduction of Allopregnanolone output is due to stress-related functional hypothyroidism and a
short-term supply of the hormone “just won’t cut it”.
A better suggestion would be to consult with a Functional or Metabolic Medicine MD, with a view to:
[1] Testing DHEA, Free Testosterone, Progesterone, Oestradiol, HSCRP, Homocysteine and IGF ( Growth Hormone indicator), then
[2] Taking DHEA, 50mg at 8AM.
[3] Taking NAC, 900mg, MTHF (vit B9) 2 mg and Magnesium Threonate 2G twice daily to reduce brain inflammation.
[4] Taking Progesterone 100 mg and Melatonin, 5-10 mg at night.
[5] Restoring T3 level with oral T3 (at 04:00AM), IF the Free T3/Reverse T3 ratio (see “Thyroid Hormone”) is lower than 24,
[6] If there is no improvement in one week, starting a one-month course of Zuranolone, to provide temporary Allo. support.
[7] Continuing MD supervision and T3 correction until the FreeT3/Reverse T3 ratio has been greater than 24 for six months.
REFERENCES
These few references have been selected from several dozen excellent “papers”: readers who need more in-depth information will find it easily by locating these references on line and looking for “similar articles”.
BEST IS # 7, “ALLOPREGNANOLONE, THE NEUROMODULATOR TURNED THERAPEUTIC AGENT”: ALSO #* & #9, RE NEW Rx.
(1) Circulating levels of allopregnanolone in humans: gender, age, and endocrine influences.Genazzani AR1, Petraglia F, Bernardi F, Casarosa E, Salvestroni C, Tonetti A, Nappi RE, Luisi S, Palumbo M, Purdy RH, Luisi M J Clin Endocrinol Metab. 1998 Jun;83(6):2099-103. PMID: 9626145 DOI: 10.1210/jcem.83.6.4905, in The Journal of Clinical Endocrinology & Metabolism, Vol 83, # 6, 1 June 1998, Pages 2099 2103, https://doi.org/10.1210/jcem.83.6.4905–
(2) The role of allopregnanolone in depression and anxiety
https://pubmed.ncbi.nlm.nih.gov/24215796/
(3) Progesterone metabolite allopregnanolone in women with premenstrual syndrome – ScienceDirect(opens in a new tab)sciencedirect.com/science/article/abs/pii/S0029784497004171#! Obstetrics & Gynecology Volume 90, Issue 5, November 1997, Pages 709-714 MDAndrea J.RapkinabcMSWMelindaMorganabcRNP, MNLindaGoldmanabcPhDDarrell W.BrannabcPhDDeborahSimoneabcPhD, DPhilVirendra B.Maheshabc
(4) Wikipedia, “Allopregnanolone”, https://en.wikipedia.org/wiki/Allopregnanolone
(5) ROLE OF ALLOPREGNANOLONE IN DEPRESSIVE-LIKE BEHAVIORS: FOCUS ON NEUROTROPHIC PROTEINS, Felipe Borges AlmeidaaMaurício SchülerNinabcHelena Maria TannhauserBarrosa, Neurobiology of Stress Vol.12, May 2020, 100218 https://www.sciencedirect.com/science/article/pii/S2352289520300084
(6) Neurosteroid biosynthesis down‐regulation, and changes in GABAA receptor subunit composition: a biomarker axis in stress‐induced cognitive and emotional impairment: Andrea Locci 1 and Graziano Pinna 1Br J Pharmacol. 2017 Oct; 174(19): 3226–3241.Published online 2017 Jun 14. doi: 10.1111/bph.13843 PMCID: PMC5595768 PMID: 28456011 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5595768/
(7) ALLOPREGNANOLONE, THE NEUROMODULATOR TURNED THERAPEUTIC AGENT:
Graziano Pinna *Department of Psychiatry, The Psychiatric Institute, University of Illinois at Chicago, Chicago, IL, United States. Front. Endocrinol., 14 May 2020 |
https://doi.org/10.3389/fendo.2020.00236
https://www.frontiersin.org/articles/10.3389/fendo.2020.00236/full
(8) Canadian provincial websites imply that Brexanolone is, or will be, available in here, but
https://myhealth.alberta.ca/Health/medications/Pages/conditions.aspx?hwid=fdb2058
(9) Zuranolone is, I think, also on track for availability in Canada: https://www.medscape.com/viewarticle/960452
