WHAT IS ALZHEIMER’S DISEASE?
Alzheimer’s disease is a slow process of cognitive decline, thought to be due to functional isolation of brain cells by progressive accumulation of waste (“Tau” and “Beta-Amyloid”) molecules in the junctions between the cells.
This accumulation may occur either by overproduction of Tau and Beta-Amyloid waste products, or by failure of the system to clear those molecules from the intercellular spaces. It is more likely that the cause is a failure in “house cleaning”, so that naturally produced waste material accumulates and aggregates, progressively clogging the system and eventually, slowing cognitive function to the point of total shutdown.
An inherited tendency (not a hard-and-fast, inevitable, progressive process) to Alzheimer’s disease has been demonstrated and while Alzheimer’s does tend to run in families, it is not possible to predict its occurrence in the vast majority of cases. It is likely however that maintenance of mental, physical and metabolic health would lead to a reduction of the incidence of Alzheimer’s disease.
PROBABLE MECHANISM OF HOUSEKEEPING ACTIVITY:
THE LYMPHATIC SYSTEM:
As the blood flows throughout the body, small amounts of water get squeezed out of the capillaries into the space between the cells (the interstitial space). This “Interstitial fluid” eventually enters the “Lymphatic system”, travelling through tiny tubes to the lymph glands and then through similar, though larger, tubes to empty into the bloodstream at the base of the neck.
THE GLYMPHATIC SYSTEM:
In the brain, there is (1) similar, passive production of interstitial fluid, amounting to about 20% of fluid production; but in addition, there is (2), active production of CSF (cerebro- spinal fluid), secreted by the Choroid plexus of micro-blood vessels in each of the four ventricles. This fluid exits through four little holes in the fourth ventricle, circulates through the brain tissue to the sub-arachnoid space and is reabsorbed by the “arachnoid”, a diaphanous tissue like spiderweb which covers the surface of the brain. The rate of CSF formation in humans is only 0.3 – 0.4 ml min, but (3) a bi-directional, pulsatile flow across the blood-brain barrier, much more rapid than the CSF flow, occurs with every heartbeat, as the arterial pressure drives fluid through the capillaries which supply the brain with oxygen and nutrients. For detail re. CSF production and flow, see “A new look at cerebrospinal fluid circulation”, by Brinker et. al., Published 01 May, 2014, at https://fluidsbarrierscns.biomedcentral.com/articles/10.1186/2045-8118-11-10
There are 4 methods by which waste products are thought to be eliminated: (1) Enzymes dissolve the waste, for transport through the blood-brain barrier (the BBB) to the bloodstream. (2) Waste product fragments are washed out: “Glymphatic” fluid enters the periarterial space from the subarachnoid area and flows to the ends of the arteries, where the sheath of the artery is “fenestrated” (hole-y). Leaking into the brain tissue through the holes, it picks up Tau and Beta Amyloid fragments and transports them to the perivenous spaces, through which it passes along the veins to the outside of the brain, emptying into the lymphatic system (see diagram). (3) Direct transfer of soluble products, to the “Meningeal” lymphatic system [“Meninges” is the name for a thin bag which the brain sits in]. (4) Glymphatic fluid carrying Amyloid and Tau fragments pass along the cranial nerves, in the perineural channels, in the same fashion as in (2).
Of these three, the major route is (1): the barrier into the glial lymphatic system is permeable to most proteins and transport of beta amyloid across the blood-brain barrier and into the meningeal lymphatics has been demonstrated experimentally.
It has been observed that during sleep, the brain and glial (supportive) cells contract, thus enlarging the spaces through which the interstitial fluid flows and facilitating more rapid flow of fluid. In mice, this space has been observed to increase by 60%, during sleep. In addition, transfer of Glymphatic fluid through the BBB also increases during sleep.
It is reasonable to assume that the root cause of Alzheimer’s disease is failure to clear waste material, rather than an increased rate of production of waste. Accumulation therefore must result from either (1) Failure of the Arachnoid to produce enough CSF, so that the flow rate is reduced (observed in old age), (2) Reduced duration and/or rate of nocturnal interstitial fluid flow due to poor sleep patterns of whatever origin, natural, pathological or chemical, (3) Obstruction of the Glymphatic channels, (4) Progesterone deficiency, leading to underproduction of Allopregnanolone and its Metabolites and consequent poor sleep, less brain cell shrinkage during sleep and reduced “cleanup” of the spaces between the cells.
IS “ALZHEIMER’S” WORSENED BY OTHER CONDITIONS? ………………. yes:
(1) Deficiency of DHEA, Testosterone, Oestrogen, Progesterone, Melatonin, Vitamin D, Magnesium, Tryptophan. (2) Diabetes, severe kidney or liver disease, alcoholism, THC overdose and metal overload, Inflammation and oxidative stress, Concussion, Mercury, Lead, Copper etc.(3) Hypothyroidism, either “true” or “functional”, which results in slowing of all body functions, including cognition.
THE BRAIN’S DRAINAGE SYSTEM: NOT so COMPLICATED, REALLY !
The purple cells are brain cells (Neurons), the bright green ones are “Astrocytes” and the light greens are glial cells. The brown granules are Tau and Beta-Amyloid waste.
The Tau and Beta-Amyloid granules are being broken up into tiny bits and pushed down the feet of the astrocytes into a space around each artery or vein, where fluid flow carries them along the surface of the vessel, to be dumped into the glymphatics and from there, into the blood. I call this process, maximised by dilation of the channels during sleep, “brain housekeeping”.
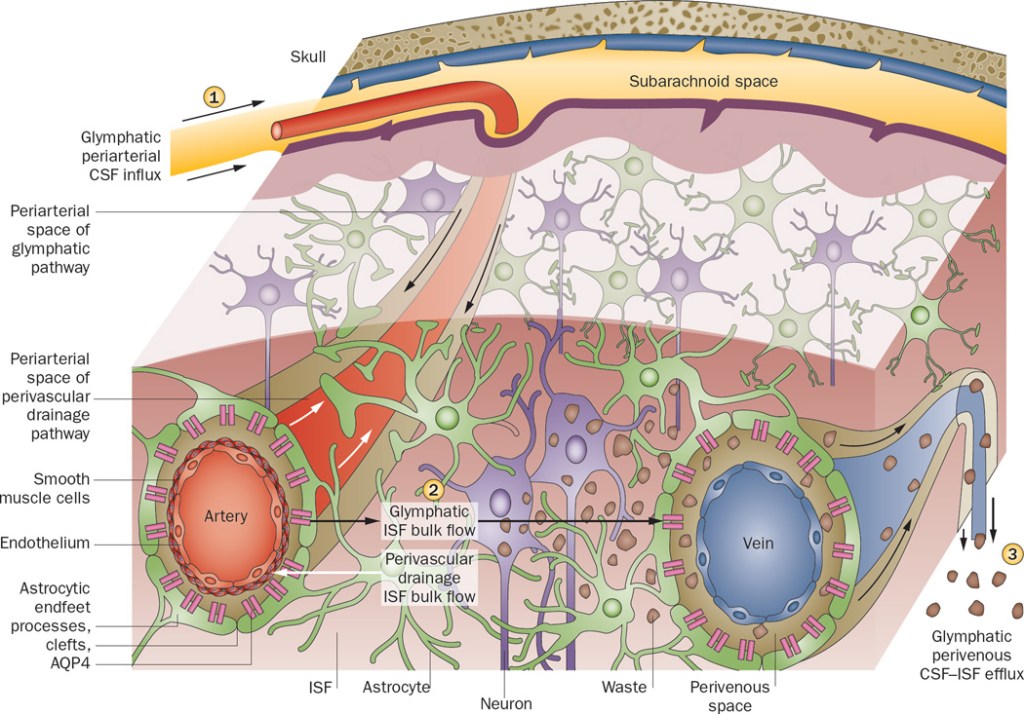
Graphic:“Interaction between blood-brain barrier and glymphatic system in solute clearance” by Verheggen, VanBoxtel, Verhey, Jansen, Backes.
THE BRAIN’S HOUSEKEEPER:
ALLOPREGNANOLONE, made from PROGESTERONE, is the brain’s most important hormone. Progesterone elevates Allopregnanolone levels with good dose-to-serum-level correlations.
Working with DHEA, Testosterone, T3, Melatonin and Magnesium, Allopregnanolone “does” brain maintenance and repair, possibly including remyelination of denuded axons in MS. It enhances self-esteem, relieves and reduces anxiety, helps produce endorphins and fine-tunes the GABA system. Thus it is neurogenic, neuroprotective, antidepressant, anti-aggressive, pro-sexual, sedative and pro-cognitive.
It takes an active role in the majntenance and repair of “Axons”, the long extensions of nerve cells which connect to other cells; but perhaps its most important function is to facilitate brain cell shrinkage during sleep. This is an all-important hedge against Alzheimer’s, because the rate of clearance of Tau and beta-amyloid from the interstitial space in the brain depends on fluid flow.
Fluid flow increases during sleep, when the brain cells (Neurons, Astrocytes and Glial cells) shrink and the passages between the cells open up. It decreases during the day, when the cells are at full volume and the passages shrink. Therefore fluid flow depends on sleeping well enough and sleeping long enough.
REMEMBER: by ensuring deep sleep, Allopregnanolone, Melatonin and Magnesium facilitate brain cleanup, reduce stress and encourage links between brain cells, thus maintaining cognitive function. Hopefully (this is unproven) enhancing brain hygeine in this way will reduce our liability to Alzheimer’s disease.
PROGESTERONE produces ALLOPREGNANOLONE, so Progesterone deficiency causes Allopregnanolone deficiency.
WHAT SPOILS SLEEP PATTERNS?
(1) Progesterone deficiency, with resultant Allopregnanolone deficiency.
(2) Melatonin deficiency.
(3) Hypothyroidism and/or Functional Hypothyroidism: inactivation of “thyroid hormone #3” slows cognition and can cause “fuzzy thinking”, “brain fog”, confusion, anxiety and depression, adversely affecting sleep patterns.
(4) Magnesium deficiency: Magnesium participates in approximately 300 chemical processes in the body and among its effects is facilitation of sleep and enhancement of sleep patterns.
(5) DHEA/Testosterone deficiency: Testosterone enhances self-confidence, thereby reducing anxiety and depression. (5) Vitamin D deficiency.
(6) Hyperthyroidism.
(7) PTSD/Depression/Anxiety.
(8) Stimulants (coffee, tea, et cetera) and late-night alcohol intake.
(9) Habit, especially late-night reading and/or TV watching.
(10) Shift work, or light (especially blue light) in your sleeping area, which lowers your Melatonin level.
(11) Pain or discomfort, either due to injury or to inflammatory conditions such as Fibromyalgia and Polymyalgia.
(12) Bowel inflammation, such as “SIBO”, IBD and Diverticulitis.
(13) Brain inflammation due to oxidative stress, which can be eliminated with oral antioxidants.
SLOWING DOWN? FUZZYHEADED? CONFUSED? – SHOULD YOU SEE YOUR DOCTOR?
MDs tend to wait, planning to treat full-blown Alzheimer’s, or those confirmed to be in the early stages of disease.
Doctors/Investigators/research people, seemingly oblivious to the idea that our systems are dependent on an interactive, orchestrated, cooperative interplay between multiple mineral, vitamin and hormonal players, tend to focus on one factor at a time, with a sort of fuzzy-headed faith in “designed” medications.
In a condition like Alzheimer’s, which manifests 30 or 40 years after it begins, these are palpable errors.
To apply the analogy of an aging automobile, would you spend billions of dollars to develop a single fuel additive to correct simultaneously failing ignition coils, spark plugs, headlamp connectors, fuel lines, brake lines, electrically operated windows, computer circuits and Generalized Rattling, or would you try maintenance and early repair, correcting each factor individually, on a preventive basis ?
Obviously, it would be better to begin surveillance of hormonal, vitamin, mineral and oxidative balances in youth, including Melatonin, DHEA, Testosterone, Progesterone, Oestrogen, Vitamins, T3 and minerals whenever deficiency begins. Correction of imbalances should begin as soon as a deficiency is found. CAVEAT: bearing in mind that many normal people deviate from the average, surveillance should include education for all subjects, encouragement re. diet and excercise, careful interpretation of symptoms, physical examination as necessary and flexible analysis of test results.
SO WHAT CAN YOU DO WHILE WAITING FOR THE MEDICAL PROFESSION TO ARRIVE AT THIS LOGICAL CONCLUSION?
(A) Follow the Guru: Read, “The End Of Alzheimer’s”, by Dr Dale Bredesen:
(B): Eat well, destress, sleep, exercise.
Eliminate simple carbohydrates, gluten and processed food, eat more vegetables, fruits and non-farmed fish.
Meditate twice a day, do yoga to reduce stress and sleep seven to eight hours per night.
(C): Be proactive: it is better to avoid health issues, than to correct them.
Take Melatonin, Methylcobalamin, Vitamin D3, Vitamin K2, Vitamin C, Vitamin B2 And Vitamin B6, fish oil, NAC and Coenzyme Q10 each day………… see the “anti-Alzheimer’s protocol” on the final page of this paper.
Optimize oral hygiene using an electric toothbrush/flosser, to minimise inflammation from migrating mouth germs.
Fast for 12 hours between dinner and a fruit for breakfast, have a light snack at lunch and then don’t eat until dinnertime.
Don’t overuse alcohol.
Exercise for 30 minutes, 4 to 6 days per week.
Consult with a bioidentical hormone restoration professional for assessment, correction and maintenance of your hormonal balance regardless of your current age, and ask specific questions based on the information in this article and your learning from Dr Bredesen’s book.
