
ABSTRACT
(brief description-this is the 2nd longest page in this website)
Alzheimer’s disease, a slow process of cognitive decline, causes progressive loss of brain cells over a very long time (30 – 40 years).
We can’t see what’s going on inside the brain cells in Alzheimer’s disease, but we can see twisted, ruined beta-amyloid piled up around and between them and and twisted, tangled tau peptides inside them: we know that they have become nonfunctional.
Beta-amyloid
We don’t know why, but “Beta-Amyloid peptide” * inside affected brain cells twists, breaks and is ejected, piling up outside of the newly nonfunctional cells.
TAU
The TAU (tubulin ** -associated unit) protein, a mesh that supports the transport and nerve-signal channels inside each affected neuron, also breaks. It twists and tangles up inside the cells, so even if the cell is still alive, the channels can no longer carry nerve signals ***.
Scientists assume that the beta-amyloid and TAU waste kills the brain cells. However it is more likely that the cells are killed by some unknown process, as a result of which beta-amyloid and tau proteins become deformed, broken and nonfunctional.
The beta-amyloid fragments are ejected from the cell and the TAU fragments tangle within: by the time we can see the accumulation of amyloid and TAU, the neuron has stopped working and is dead, or dying.
Whatever the process, affected cells are lost from the brain’s working population: brain cells die and are removed by the brain’s clean-up process.
* Peptides are short “chains” of amino acids, with which proteins are built.
** The walls of the “microtubules” that carry nerve signals are made from Tubulin, a special protein built from “tubulin associated unit” peptides.
*** When a nerve cell is deteriorating in Alzheimer’s disease, the Microtubules are destroyed and the Tubulin Associated Unit (TAU) peptides that make up its walls are released.
Cognitive decline
Cognitive decline is masked by ad hoc “rewiring” until severe damage has been done.
The brain can do “workarounds” and reconfigure itself, continuing to think and respond to the surroundings, even when more than 50% of its working population of brain cells has disappeared. So by the time we realize that someone has Alzheimer’s disease, some 70% of the brain cells have died and been reabsorbed.
Amyloid-removing medications
Recently, the pharmaceutical industry has designed medications that can speed up removal of beta-amyloid. However logically, the hope that removing amyloid will “cure” Alzheimer’s disease is wasted thought: the disease is due to the cells dying, not to blocking of signals from living cells.
Furthermore, the collection of beta-amyloid waste which we see around the cells isn’t just sitting there: it is being actively removed, but the “brain’s housekeeper”‘ can’t move it fast enough.
Anyway by the time dementia starts, we can see that the brain is shrinking (figure 1): by the time we notice a problem, 70% of our 86 billion brain cells (neurons) have died and been reabsorbed, so cleanup drugs can do nothing except slow the progress of disease. “Curing” Alzheimer’s disease would involve regenerating a significant portion of the missing brain cells, and that is a faint hope, indeed.

Figure 1
Normal, vs. Alzheimer’s brain
https://en.wikipedia.org/wiki/Alzheimer%27s_disease
Below, I outline our knowledge of the brain, the cleanup process and Alzheimer’s disease. I recommend books, by smarter people than myself, to improve your “self-help-ability”. I make some guesses and assumptions about how beta-amyloid and tau are damaged and I make some suggestions as to what we can do to prevent the process or, slow it.
However as you will realise, I can offer only my opinion, gleaned from others’ research and from my (hopefully) logical thinking about the problem. My statements should not be taken as “gospel truths”: rather, you should view them as good ideas that you can use to understand the problem and perhaps, come up with a solution, yourself.
Please see the final section of this monograph, entitled “SLOWING DOWN? FUZZYHEADED? CONFUSED? – SHOULD YOU SEE YOUR DOCTOR?” …
Skim through everything in between, if you wish, but you must read that final chapter! Otherwise, you could get Dr. Dale Bredesen’s book, “the end of Alzheimer’s” and read that, instead, but this article will take you less time.

WHAT IS ALZHEIMER’S DISEASE?
Alzheimer’s disease is a slow process of cognitive decline, which takes three to four decades to develop.
It is thought to be due to functional isolation of the brain cells (neurons) by progressive accumulation of broken, mis-folded (twisted) “Beta-Amyloid” in the junctions between the cells and to breaking and “tangling” of tau protein strands in the walls of the “microtubules”, the transport channels of the Cells.
However, in my opinion the twisted tau in the brain cells and the beta-amyloid surrounding them are the result, not the cause, of disease within the neurons.
Beta-Amyloid
We don’t know exactly what beta-amyloid does, but according to Wikipedia, normal beta-amyloid may activate kinase enzymes, reduce oxidative stress, regulate cholesterol transport and protect against infection. We don’t know either, why beta-amyloid is ejected from the neurons: all we know is that the junk we see isn’t normal.
In any event, in Alzheimer’s disease, beta-amyloid accumulates in plaques (lumps) around the neurons, and the brain shrinks as the neurons die and are cleared away.
Tau protein?
According to Wikipedia, TAU (Tubulin-Associated Unit), a group of six soluble proteins, forms a thin scaffolding which maintains the stability of tiny microtubules (MTs) in all cells, including neurons. These microtubules extend all the way along the axons, some of which are in length. MTs assemble into long (up to a metre or more), semi-rigid structures which act as conduits for the transport of chemical and electrical signals in the cell and its extensions, the dendrites and axons. MT-based transport plays an important role in the function of all cells, including astrocytes, oligodendrocytes and nerve cells outside of the CNS.
In Alzheimer’s disease, the microtubules are destroyed: the TAU protein filaments in their walls twist, break, tangle, and accumulate in the cell. The reason for this hasn’t yet been explained; but some metabolic aberration must be at fault and possibly, cell maintenance has gone awry due to hormone deficiency, or unavailability of some nutrient or vitamin.
Alzheimer’s Shrinking brain
In Alzheimer’s disease, the cause of perhaps 70% of cases of dementia, axons are destroyed and neurons die, in no particular area or pattern, across the brain.
Affected brain areas shrink and cognitive function slows and deteriorates (Fig 1).
Alzheimer’s sufferers variably exhibit memory loss, attention deficit, aberration of reasoning, mood swings, temporal and spatial disorientation, psychological effects, and eventual loss of balance and coordination. All of these vary, in timing and degree, from person to person; but eventually, the personality and the ability to engage with others disappears as the disease progresses.
Inheritance, Alzheimer’s:
1–2% of Alzheimer’s disease cases are inherited; affected individuals show changes at a much younger age and the disease progresses more rapidly. Three single-gene mutations are associated with this condition: a chromosome 21 gene for “amyloid precursor protein” (APP), a chromosome 14 gene for “presenelin1” and a gene for “presenelin2”, on chromosome #1. However, while age-related Alzheimer’s tends to run in families, it is not possible to predict its occurrence in the majority of cases.
What does an inherited gene actually do?
Caveat: (my opinion).
There is some question as to whether an abnormal gene produces its effects as a de facto function of its existence, or whether it simply renders its target organ more susceptible to the deleterious effects of hormonal, essential amino acid, vitamin or essential element deficiency: if the latter, a serious question is implied: could the effects of the gene be averted by supplying the deficient item in adequate quantity?
THE HOUSEKEEPERS
Water management in the body as, a whole:
As the blood flows around the body, a little water leaks through microscopic holes in the capillaries, into the “interstitial” space between the cells. This Interstitial fluid, called “lymph”, travels through tiny “lymphatic” tubes to the lymph glands and then through larger tubes to empty into a vein at the base of the neck.
This system serves the entire body, including the scalp, face and skull, but the brain has its own waterways which, for want of a better term, make up the “glymphatic system”.
The brain’s waterways – the glymphatic system
Much of the brain’s glymphatic (“fluid”) flow is actively-produced cerebro-spinal fluid (CSF), secreted by the “Choroid” plexus of micro-blood vessels, a collection of special “ependymal” cells, surrounding a core of capillaries and connective tissue, in each of the four ventricles of the brain. This fluid exits through four little holes in the fourth ventricle and from there, it circulates through the brain tissue to the sub-arachnoid space.
Much of it is reabsorbed by the “arachnoid“, a diaphanous tissue like spider-web, which covers the surface of the brain, but some exits through the periarterial and perivenus spaces (see figure 3).
{kind=link}
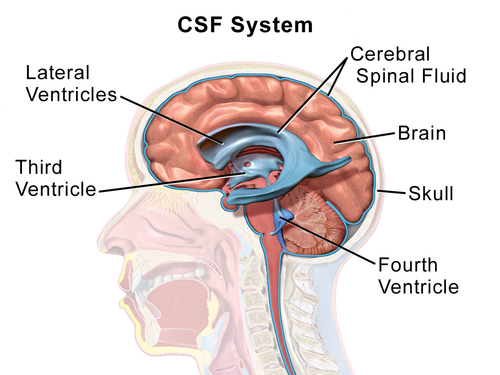
Figure 3: The ventricles, courtesy of Wikipedia
(Click “ventricles”, above this graphic, for Wikipedia’s animated depiction of the ventricles!)
The rate of CSF formation by the choroid is only 0.3–0.4 ml per minute, but there are two other sources of fluid flow:
(1) A bi-directional, pulsatile flow of fluid, across the blood-brain barrier*, occurs with every heartbeat (the link shows Wikipedia’s animated depiction of the flow).
(2) Lymph, amounting to about 20% of the total “glymphatic” fluid, produced by leakage from the capillaries which deliver blood to the brain cells.
{kind=link}
Brain housekeeping
There are four methods by which waste products are eliminated from the brain:
(1) Enzymes dissolve them, for transport through the blood-brain barrier (the BBB) to the bloodstream.
(2) Small fragments are washed out: “Glymphatic” fluid enters the periarterial* spaces from the subarachnoid area and flows to the ends of the arteries, where the sheath of the artery is fenestrated (leaky). There, it passes into the brain channels and flows around the brain cells.
Then it enters the perivenous* spaces, taking beta-amyloid fragments with it.
Travelling along the veins via the perivenous channels to the outside of the brain, it empties into the lower body’s lymphatic system (figure 5).
(3) There is also direct transfer of fluid to the “Meningeal” lymphatic system (“Meninges” is the name for the thin “bag” in which the brain sits): the Meningeal lymphatic flow joins the bloodstream, at the base of the neck.
(4) Some glymphatic fluid carrying Amyloid and Tau fragments also passes along the cranial nerves, in the perineural* channels, in the same fashion as in (2). This explains why Tau and amyloid fragments can be found in the blood, in Alzheimer’s disease.
* “perivenous” means “around the veins”, “periarterial means “around the arteries.” and “perineural” means “around the nerves”.
Of all the above drainage methods, the major route is via the meningeal lymphatics.
The importance of sleep:
During sleep the transfer of Glymphatic fluid through the blood-brain barrier increases and the brain and glial cells contract, enlarging the spaces between the cells and allowing more rapid flow of fluid. In mice, this space has been observed to increase by 60%, during sleep.
Accumulation of beta-amyloid
Assuming that the cause of beta-amyloid accumulation is failure to clear waste material quickly enough, in the face of increased waste production, accumulation must result from
(1) Failure of the Arachnoid to produce enough CSF, so that the flow rate is reduced. This happens in old age, but is a minor factor, since the CSF is only 20% of total brain fluid flow.
(2) Reduced duration and/or rate of interstitial fluid flow at night, due to poor sleep: this is significant, because sleep patterns deteriorate with age.
(3) Obstruction of the Glymphatic channels (not likely).
(4) Progesterone deficiency, leading to underproduction of Allopregnanolone, and/or
Melatonin deficieny.
Because Progesterone, Allopregnanolone and Melatonin facilitate brain cleanup by putting us to sleep and promoting brain cell shrinkage, deficiency of these hormones is a significant debility. Most likely this is the major problem, since production of these important hormones is reduced progressively, beginning in the 4th decade of life, to 20% or less of what it was In the third decade.
Is Alzheimer’s disease worsened by other conditions? … Yes ! … Here’s a list:
(1) Deficiency of any combination of DHEA, Testosterone, Oestrogen, Progesterone, Melatonin, Vit. D, Magnesium, essential Amino acids, Selenium, Iodine, Iron, Zinc, Vitamins, dietary factors Etc.
(2) Diabetes, kidney or liver disease, with chronic inflammatory cytokine production,
(3) THC overdose, smoking, alcoholism and other addictions,
(4) Severe concussion, or multiple minor concussions (for example, in sports),
(5) Mercury, Lead, Copper, Nickel and other “heavy metal” overload,
(6) Other toxins, including “forever chemicals”, like phthalates, BPA and artificial sweeteners,
(6) Inflammation, and/or oxidative stress, of the brain,
(7) True hypothyroidism,
(8) Stress-related intracellular hypothyroidism, due to stress from chronic illness, poverty, social conditions, mental illness, depression, PTSD, grief, etc.
(8) Maternal Hypothyroidism (either “true”, or “Intracellular”) in the first 20 weeks of pregnancy, causing fetal brain “miswiring”.
!
Figure 4 shows the GLIAL cells (oligodendrocytes, astrocytes, ependymal cells, and microglia), in the brain and Schwann cells and satellite cells in the peripheral nervous system.
Figure 4: GLIAL CELLS

Glial cells have four main functions:
(1) surround neurons and hold them in place;
(2) supply nutrients and oxygen to neurons;
(3) insulate one neuron from another;
(4) destroy pathogens and remove dead neurons.
In the fabulous diagram by Verheggen, VanBoxtel, Verhey, Jansen, & Backes (Figure 5), the purple cells are brain cells (Neurons), the bright green ones are “Astrocytes” and the light greens are glial cells.
The brown granules are Tau and Beta-Amyloid waste, which are being broken up into tiny bits and carried down the feet of the astrocytes into a space around each vein.
Fluid flow carries them along the surface of the vein, to be dumped into the glymphatics and from there, into the blood.
This “brain housekeeping” is maximised during sleep, when the channels dilate due to the influence of progesterone and Allopregnanolone (as said above) and the fluid flow is faster.
Figure 5: “Interaction between blood-brain barrier and glymphatic system in solute clearance”, by Verheggen, VanBoxtel, Verhey, Jansen, Backes.

Brain maintenance and repair:
ALLOPREGNANOLONE, the putative “King of the neurosteroids”made from progesterone, is the brain’s main repair hormone.
Allopregnanolone enhances self-esteem, relieves and reduces anxiety, counters stress, prevents depression, helps produce endorphins to moderate pain and fine-tunes the GABA system. It is Described by Wikipedia as “neurogenic, neuroprotective, anticonvulsant, antidepressant, anti-aggressive, pro-social, pro-sexual, sedative and pro-cognitive”.
In addition, it improves memory and works with T3 to maximize cognition.
Along with MTHF (vitamin B9), vitamin B12, DHEA, Testosterone, progesterone, T3, Magnesium, and (particularly) Melatonin, Allopregnanolone “does” brain maintenance and repair.
It takes a prime role in the majntenance and repair of “axons”: it actively remyelinates denuded axons in MS and other demyelinating conditions and it facilitates synapse repair in neurological diseases.
However, perhaps its most important functions is to shrink brain cells during sleep, as explained above.
Figure 6: Allopregnanolone: An overview of its synthesis and effects,
by S Diviccaro, L Cioffi, E Falvo, S Giatti…
J Neuroendocrinol. 2022 Feb; 34(2): e12996, 2021Jun29, doi: 10.1111/jne.12996
The Neuroprotective effects of allopregnanolone.

Therapy with Allopregnanolone
Treatment with this neuroactive steroid shows:
(A) beneficial effects on spinal cord trauma,
(B) facilitation of synapse formation and prevention of neuronal death,
(C) reduction of cholesterol accumulation,
(D) decrease in epileptic events,
(E) beneficial effects on nervous damage induced by diabetes mellitus,
(F) protective effects in neurodegenerative diseases (eg, Alzheimer’s disease, Parkinson’s disease, amyotrophic lateral sclerosis),
(G) anxiolytic and anti‐stress actions,
(H) effects against the neurotoxicity exerted by human immunodeficiency virus (HIV),
(I) protective effects in an experimental model of Niemann‐Pick disease, type C,
(J) protective effects in neuroinflammatory conditions, like multiple sclerosis and experimental autoimmune encephalomyelitis,
(K) painkilling effects against neuropathic pain.
Allopregnanolone’s helpers
Ideal maintenance and repair of the brain and the nervous system can be perfect only if there is adequate hormonal balance, but the important actors are
– Pregnenolone, which helps with axon and microtubule formation and converts to progesterone.
– Progesterone, acting as an anti-inflammatory, supports mitochondrial function, is necessary for neurogenesis and regeneration, and converts to Allopregnanolone.
It actively promotes myelination and recovery from traumatic brain injury, but much of its action is via conversion to Allopregnanolone.
– Melatonin, the body’s best antioxidant, scavenges reactive oxygen and nitrogen species, increases antioxidant defenses, prevents tissue damage and blocks pro-inflammatory cytokines. Melatonin is active in repair processes, especially remyelination.
– BDNF (Brain-derived neurotrophic factor), a nerve growth factor, aids with cell development and repair.
– Thyroid 3 (T3, “Triiodothyronine”) improves the efficiency of all cells. It is indispensable for neurogenesis, neuronal and glial cell differentiation, and normal brain “wiring” in the fetus.
Recently, animal experiments have proven T3’s effectiveness in remyelination in multiple sclerosis. A clinical trial of triiodothyronine (T3), in MS, is being done (2022).
– DHEA, the common precursor of testosterone and many “micro-hormones”, is an active player in the maintenance of all cells: Among its jobs in the brain, it promotes remyelination in MS and other neurological diseases. Some of its effect is probably attained via improvement in intracellular T3 levels, but that suggestion is as yet unproven.
– Testosterone is also essential for myelination: testosterone favors astrocyte recruitment and spontaneous oligodendrocyte-mediated remyelination.
Testosterone plays major roles in the viability, functions, and plasticity of neurons, and is also a key regulator of the myelination of axons.
– Vitamin D has protean effects throughout the body. Vitamin D helps to regulate nerve growth factor (NGF). NGF is responsible for the growth and survival of neurons, so vitamin D is essential for brain cell and nerve maintenance and repair.
Clinical pearls to remember
By ensuring sleep, Allopregnanolone, Melatonin and Magnesium “do” brain cleanup, reduce stress and strengthen brain cells, thus protecting cognition.
Pregnenolone keeps the axons and microtubules healthy and converts to progesterone.
PROGESTERONE converts to ALLOPREGNANOLONE: 100-300 mg of progesterone at bedtime facilitates sleep, by boosting Allopregnanolone production.
DHEA is the raw material for “micro-hormones” in all cells. It converts to Testosterone and a long list of local micro-hormones. Particularly, it helps with production of T3 inside all the body’s cells.
Testosterone helps with brain maintenance, maintains self-confidence, prevents anxiety and depression, preserves heart muscle function and converts to Estradiol.
Estradiol maintains the female organs, strengthens the bones and subserves many functions in the CNS, including fine motor control, learning, memory, sensitivity to pain and motor coordination.
Vitamin D has neuroprotective effects including clearing amyloid, maintaining cognition and facilitating “neuroplasticity”.
In short, keeping your hormones in balance minimises the deterioration of nerve cell health, which leads to Alzheimer’s and other degenerative diseases.
SLEEP
WHAT SPOILS SLEEP PATTERNS?
(1) Progesterone deficiency, with resultant Allopregnanolone deficiency.
(2) Melatonin deficiency.
(3) Stress-related, Intracellular Hypothyroidism (IH). Deficiency of triiodothyronine (thyroid hormone #3, “T3”) in brain cells reduces their efficiency, causing “fuzzy thinking”, “brain fog”, confusion, anxiety, depression and poor sleep.
(4) Hyperthyroidism, or “true” Hypothyroidism.
(5) Magnesium deficiency: Magnesium participates in approximately 300 chemical processes in the body. It facilitates sleep and enhances sleep patterns.
(6) DHEA/Testosterone deficiency: DHEA and Testosterone enhance self-confidence, reduce anxiety and depression and prevents “churning thoughts”.
(7) Vitamin D deficiency.
(8) Stress-related PTSD/Depression/Anxiety (causing IH).
(9) Stimulants (coffee, tea, et cetera) and late-night alcohol intake.
(10) Habit, especially late-night reading or TV watching.
(11) Shift work, or light (especially blue light), which lowers the Melatonin level.
(12) Pain or discomfort, injury or inflammations like Fibromyalgia and Polymyalgia.
(13) Brain inflammation due to “inflammatory cytokines”, such as IL-6, produced by inflamed bowel, as in “SIBO“*, Crohn’s disease, IBD and Diverticulitis.
(14) Brain inflammation due to oxidative stress, (eliminated with oral antioxidants).
(15) Psychological stress.
* “SIBO” – Small Intestinal Bacterial Overgrowth (small intestine infection).
THE ONLY WAY TO GO
SLOWING DOWN? FUZZYHEADED? CONFUSED? – SHOULD YOU SEE YOUR DOCTOR?
MDs wait, to treat full-blown Alzheimer’s, or patients in the early stages of disease.
Most doctors, Investigators and researchers seem not to understand that our systems depend on an interactive, orchestrated, cooperative interplay between multiple mineral, vitamin and hormonal players.
They focus on one factor at a time, with a fuzzy-headed faith in synthetic “designer” medications, none of which has proven effective in treating Alzheimer’s disease.
In Alzheimer’s, which manifests 30 or 40 years after it begins, this is a mistake. Alzheimer’s is like a thief in the night: by the time you realize that there is a problem, your most precious cognitive “belongings” are gone.
Therefore Proactive, anticipatory care, with early identification and correction of the multiple dietary, vitamin, mineral and hormonal aberrations to which we are subject, is the only way to go. we should support and repair our hormonal balance, so as to give the body’s maintenance and repair systems their best possible chance to prevent nerve cell deterioration.
Let’s apply the analogy of an aging automobile:
Would you spend billions of dollars to develop a single fuel additive to correct simultaneously failing ignition coils, spark plugs, headlamp connectors, fuel lines, brake lines, electrically operated windows, computer circuits and Generalized Rattling?
…… and ……
If you did develop a single additive, would you wait until everything was falling apart before putting some into your gas tank?
Wouldn’t it be better to do regular maintenance, repairing defects as soon as they are found, so that you never have to face rotten, irreplaceable parts, after a total breakdown?
Obviously, it would be better to begin surveillance of hormonal, vitamin, mineral and oxidative balances while we are young, beginning to supplement Melatonin, DHEA, Testosterone, Progesterone, Oestrogen, Vitamins, T3, Magnesium, Selenium, Iodine and other essentials as soon as deficiency is found.
Surveillance should include education for everyone.
Doctors should advise re. diet and exercise, watch carefully for symptoms and do physical examination and tests as necessary. We should all be enrolled in a proactive, preventive care program, in which scheduled “checkups” include hormone and thyroid balance tests, tailored to the individual.
Q: WHAT CAN YOU DO WHILE WAITING FOR THE MEDICAL PROFESSION
TO ARRIVE AT THIS LOGICAL CONCLUSION?
A: Try the ANTI-ALZHEIMER’S PROTOCOL, based on Dr. Bredesen’s principles:
– Check your hormone, vitamin and mineral balances once a year.
– Test for heavy metal overload, every five years, and do chelation if necessary.
– Particularly, monitor DHEA, Testosterone, Oestradiol, Progesterone, Thyroid3, Thyroid4, reverse T3, TSH, and vitamin D and supplement those hormones, as necessary.
– Don’t forget the Vitamins: B12, Methyl Tetra Hydro Folate (MTHF, Vitamin B9), etc.
– Do urine tests for Minerals, especially Iron, Calcium, Magnesium and Zinc.
– Maintain Cholesterol and Glucose Levels (they improve when IH is corrected).
– Rule out inflammation, with ESR, HSCRP and Homocysteine, (Homocysteine goes up with brain inflammation, and is easily corrected with MTHF).
– Check for arteriosclerosis (hardening of the arteries produced by calcium)
– Investigate strange symptoms like hoarseness, constipation, brittle fingernails and thinning eyebrows.
– Correct any deficiencies on an ongoing basis, so as to provide your brain with the metabolic mileiu it needs for efficient housekeeping.
B: Follow the Guru:
– Read “The End Of Alzheimer’s”, by Dr Dale Bredesen and “DHEA in Human Health and Aging“, by Ronald Ross Watson, PhD.
– Read “DHEA”, “testosterone”, “progesterone” “Allopregnanolone”, “Intracellular Hypothyroidism” etc., in this website (if you haven’t already read them).
– Destress: meditate, listen to music, dance if you want to, do yoga and sleep 7-8 hours per night.
– Sleep, exercise and eat well: eliminate simple carbohydrates, gluten and processed food, eat more vegetables, fruits, nuts and non-farmed fish.
– Be proactive– it’s better to avoid problems, than to correct them: DHEA 50 mg, progesterone 100 mg (men), progesterone 2–300 mg (women) will help all systems.
– Take Melatonin, Vitamins B12, D3, K2, C, B2, B6, fish oil, MTHF, NAC, IC3 and CoQ10 each day.
– Optimize oral hygiene, using an electric toothbrush and floss.
– Fast for 12 hours after dinner, have a fruit, with coffee or tea, for breakfast, a light snack at lunchtime and whatever you like, at dinnertime.
– Don’t overuse alcohol.
– Stop smoking.
– Exercise for 15-30 minutes, 3 to 6 days per week.
– See the “anti-Alzheimer’s protocol” on the final page of this paper. *****
– Consult with a functional medicine or bioidentical hormone professional and ask questions, based on this article and/or the books by Dr. Bredesen and Dr. Watson.
***** Most people who have a “normal” diet, including “veggies”” and fruit, moderate protein, eggs, milk etc. don’t NEED supplemental vitamins for maintenance purposes. However it’s smart to add the list (below) to the diet: just don’t take the full dose as recommended on the bottle if you are healthy.
For example the dose of MTHF (Vitamin B9) for someone with Alzheimer’s brain inflammation and a high Homocysteine is 3-5 mg per day; but for a healthy person just 1 mg per day is enough to correct a small dietary deficiency.
ABOUT SUPPLEMENTS which help to prevent Alzheimer’s disease:
Melatonin is chronobiotic, hypnotic, anxiolytic, analgesic, pro-cognitive and antidepressant. It runs our biological clock, dictating hormone release times. Production falls 10% per decade, so at 50, it is ½ and at 80, it’s 1/10, of what it was at age 20: you can take 1 – 10 mg of melatonin.
If it makes you groggy in the morning, take less. (Webber’s “super sleep” contains just 1.5 mg of melatonin and works very well for sleep).
DHEA, Pregnenolone, Progesterone, Estradiol, Thyroid 3 and the FT3/reverse T3 ratio, should all be checked at least yearly, from age 25. Balancing supplements should be prescribed for deficiencies.
Vitamin B12 (Methyl Cobalamin) supports brain and nerve function, facilitates iron absorption, enhances immune system function, controls oxidation, boosts energy and helps memory.
It is in fish, meat, poultry, eggs, and dairy products, but isn’t absorbed from food if stomach acid production is too low (or is blocked by drugs).
It should be tested: it can go too high, which might mean that you have a blood abnormality and you should see your doctor: if you don’t need it, don’t take it.
Take 1 mg (1000 µg) of Methylcobalamin daily, if you need it.
Vitamin C, from fruit and vegetables, works with Vitamin D to block infections. It is necessary for wound healing and many other maintenance jobs in the body. It also does some interesting things, like helping to prevent hardening of the arteries.
Dogs and other “lower” animals make Vit.C naturally, but we don’t. The Vit-C guru, Linus Pauling, recommended 9 G/day and present-day Naturopaths give up to 50G intravenously, for viral infections, or maintenance we only need two grams a day, approximately.
Vitamins C is excreted quickly in the urine, so we need to get it from our food every day.
Take one gram twice a day and double the dose if you get a cold, a large wound or a surgical operation.
Vitamin D3 is a fat-soluble hormone made by the skin (up to 40,000 units in 24 hours).
It regulates calcium, phosphorus and bone maintenance, helps the immune system, maintains calcium for muscle function, helps the brain’s maintenance and repair, produces Cathelicidins and Defensins (natural antibiotic/antivirals) and is an anticancer agent. Fish oil contains large amounts of D3.
The dose is 2000 – 5000 iu of Vitamin D3 daily, but get your doctor to test it, to ensure that you are not taking too much (the normal level is 75 – 250 ng/ml).
Vitamin K2 is fat-soluble and is best combined with vitamin D.
Gut bacteria produce it from “leafy greens” and it is present in fatty foods, like egg yolk and high-fat dairy from grass-fed cows.
It is essential for blood clotting, bone maintenance and heart health and it reduces blood vessel calcification (arteriosclerosis).
It reduces spinal fractures by 60%, hip fractures by 77% and other fractures by 81%.
Combined D3/K2 is available in a single capsule.
Take 150 µg of Vitamin K2, daily.
Vitamin B9 (Folic acid) is best taken as MTHF (MethylTetraHydroFolate).
It is needed to make red and white blood cells in the bone marrow, to convert carbohydrates into energy and to produce DNA and RNA.
However the “biggie” is that It soothes brain inflammation, and we can tell that it is working because it reduces the Homocysteine level in the blood.
MTHF is in fruit, leafy greens, beans and seeds, seafood, but not in meat, except liver.
Take 1µg of MTHF (Methyl Tetrahydrofolate) daily: if Homocysteine is high, take 3 µg (in some situations, your functional medicine MD might prescribe 5 µg a day).
Caveats, regarding MTHF:
(A) Preparations of MTHF have labels which will seem strange to you.
To read them, you have to understand the following concepts:
(1) “S” stands for “sinister”, the Latin for “left”, while “D” means dextro, Latin for “right”.
(2) L (Levo), or S (Sinistro), means that the molecule of MTHF is “left-handed” (twisted anticlockwise): “Left-handed” MTHF, labelled “S”, or “L” MTHF, is biologically active.
This is the form of MTHF that humans need.
You can take it if the label says L-Methylfolate, 5-methyltetrahydrofolate, (6S)-5-methyltetrahydrofolate, Quatrefolic, 5-MTHF, L-5-MTHF, Metafolin, Deplin, or Levomefolic acid.
(3) MTHF labelled R (right) or D (dextro) is not biologically active: it is “right-handed” (the molecule is twisted clockwise) – it is not the form of MTHF that humans need.
If the label doesn’t say Metafolin, L-Methylfolate, or Quartrefolic, it’s probably not biologically active for humans.
People with severe methyltetrahydrofolate reductase (MTHFR) deficiency cannot make 5-MTHF. They need a higher dosage (nominally, 3 mg a day).
It’s possible to take too much MTHF: the side effects are severe anxiety, nausea, insomnia, migraines, irritability, achy joints, headache, rash, acne, fatigue, dry mouth, palpitations and sore muscles.
NAC (N-Acetyl Cysteine) stimulates glutathione, to increase the efficiency of the Mitochondria all over the body, including the brain.
Take 900 µg of NAC daily (the full dose, if needed, is 1800mg).
I3C (Indole-3-carbinol) is anticarcinogenic, antioxidant, and anti-atherogenic.
Take 200 mg of I3C daily.
Coenzyme Q 10 is a nutrient that occurs naturally in the body and in many foods.
CoQ10 is antioxidant, is needed for heart maintenance, delays Alzheimer’s disease, and is anti-inflammatory.
You must replace CoQ10 if you take Cholesterol-lowering drugs: they destroy CoQ10.
The daily dose is 200 mg.
Vitamin B6 is water-soluble, helps with more than 100 enzyme reactions and with reducing homocysteine. You need it to make hemoglobin, for brain health and anti-inflammatory action.
It repels mosquitoes, in some people.
25 mg B6, daily, is adequate.
Vitamin B2 (riboflavin) is water-soluble.
B2, 10 mg daily, is necessary for energy, care of brain and nerves, absorbing other vitamins, hormone production and other functions.
NOTE: “Multivite” pills contain combinations of the above: check the labels and
“mix & match”, to take fewer pills.
HORMONES:
Everyone over 30 years of age needs DHEA: 50mg daily maintains muscle, protects the heart from dysrhythmia and infarction, prevents or retards many cancers, treats sexual dysfunction in the female, helps with self-confidence and reduces anxiety.
In men, it raises Estradiol levels, preventing bone loss, slowing wrinkling and keeping the bones stronger.
It also reduces stress by lowering cortisol and raising the intracellular T3.
Men over 50 need Progesterone, 50-100 mg at bedtime: women need 100-300mg.
Every postmenopausal woman needs Oestradiol and Oestriol (the requirement is variable, from individual to individual): it is best applied as a cream, from a compounding pharmacy.
Every living human cell needs an optimal intracellular supply of triiodothyronine (“T3”). Get tested for TSH, T4, T3 and reverse T3: if the ratio between T3 and rT3 (T3/rT3) is less than 20, you need treatment with slow-release T3.
Note: the regular family doctor and the endocrinologist do not usually understand the T3 problem: read “intracellular hypothyroidism” in this website, and consult with a knowledgeable family doctor, or a “metabolic”, “functional” or “HRT” MD.